Atrial fibrillation
Atrial fibrillation is the most common heart rhythm disorder. It causes rapid and irregular contraction of the atria. The atria thus lose the function of creating the heart rhythm and the function of filling the ventricles. The rhythm is then irregular, usually faster and responding differently to load, and the performance of the heart is reduced with poorer ventricular filling. However, this is not an immediately life-threatening condition because the fibrillation cannot move to the ventricles. The ventricles are separated from the atria by the specialized tissue of the atrioventricular node, which delays the excitation and thus the vital function of ventricles is preserved.
-
Irregular chaotic fluttering of the atria
-
Age
Male gender
Obesity
High blood pressure
Diabetes mellitus
Sleep apnoea syndrome
Alcohol
-
At least a single-lead ECG with documented atrial fibrillation is needed for diagnosis
Classical ECG
ECG by smartwatch
Holter ECG
-
They can be diverse, some perceive the arrhythmia very unpleasantly, others may not observe it
Palpitations - irregular, rapid beating or fluttering of the heart
Fatigue
Underperformance
Exertional dyspnoea
Chest pain
-
Influence of risk factors - obesity, high blood pressure, diabetes, sedentary lifestyle
Anticoagulation - prevention of thromboembolic complications
Rhythm control or frequency control to improve quality of life

In atrial fibrillation, chaotic electrical activity of the atria with irregular transmission to the ventricles by the atrioventricular node
The risk of atrial fibrillation increases with age. In addition, this rhythm disorder (or arrhythmia), is more common in obese individuals, in cases of untreated high blood pressure or diabetes, and in patients with heart failure. There is also a higher risk in patients with increased thyroid function, ongoing infection or shortly after surgery. Alcohol excess can also be a trigger. If one of these causes is eliminated or treated, the risk of arrhythmia is also reduced. It is reported that if an obese patient with high blood pressure loses weight and is treated for high blood pressure, the effect on reducing the risk of recurrent atrial fibrillation is similar to that after treatment with catheter ablation. However, atrial fibrillation can also occur in a young, active and otherwise healthy individual. This shows that the risk is also largely determined by heredity.

Obesity and hypertension are risk factors for atrial fibrillation
In atrial fibrillation, patients often experience an irregular and rapid heartbeat. It may have the character of trembling or the sensation of fluttering butterfly wings. However, each individual is differently susceptible, and while some describe this condition as distinctly unpleasant, others may not notice the change in the beating at all. Very often, however, poorer performance, fatigue or shortness of breath on exertion is present. This can be very limiting for young active individuals. Conversely, in older individuals and those with a number of other limiting conditions, the contribution of atrial fibrillation to the overall condition may not be as pronounced and even after restoration of the natural rhythm, there is no significant improvement in quality of life. Relief of the discomfort may also occur if medication slows the conversion to ventricular pacing, even though atrial fibrillation persists. In atrial fibrillation, some patients may experience chest pain, even if the heart is otherwise healthy.

Palpitations, or the sensation of heart palpitations, can be perceived with varying intensity in atrial fibrillation
To confirm the diagnosis of atrial fibrillation, it is necessary to detect this arrhythmia on an electrocardiogram (ECG). This is easy if the arrhythmia is persistent and can be difficult if the atrial fibrillation is intermittent (paroxysmal) and ends before the ECG can be recorded. Currently, the possibility of using smart electronics to record the ECG is an advantage. For example, some smartwatch models can record a good quality single lead ECG from which an accurate diagnosis of atrial fibrillation can be made. On the other hand, it is not yet possible to base a diagnosis solely on heart rate irregularities, which can be continuously monitored and evaluated by smart watches or fitness bracelets, even with the help of artificial intelligence. In these cases, they can only alert to the possibility of atrial fibrillation, but the diagnosis must always be subsequently confirmed by capturing the arrhythmia on an ECG. If intermittent atrial fibrillation is suspected, an outpatient cardiologist can perform a so-called Holter ECG, in which the ECG is monitored continuously for 1 to 7 days. If there are difficulties, for example, only once a month, the outpatient cardiologist may issue a so-called episodic ECG recorder, which the patient puts on his or her chest at the time of difficulty.

Single-lead ECG recording by smartwatch.

Holter ECG

ECG curve with detection of atrial fibrillation - atrial contractions are not evident and the rhythm is irregular.
As such, atrial fibrillation probably shortens life slightly. However, the data showing this are from patients who were not known to have been treated well. At the same time, we know that in countries with advanced health care, the risk of death in patients with atrial fibrillation is much lower than in countries with less developed health care. It can therefore be assumed that in properly treated patients, life expectancy will be only minimally affected by the arrhythmia itself.
So what is the treatment for atrial fibrillation? The most important thing is protection against stroke. This can be achieved with drugs that reduce blood clotting - anticoagulants. The fibrillating left atrium does not contract effectively and so blood flows less easily in it. If the blood stays in the atrium longer, it can start to clot and form clots, or thrombi. This happens especially in the left atrial appendage, which has many folds and is most likely to reduce flow. The blood clot can then float, or embolise, into the arteries feeding one of the organs. Embolization is most common in the brain because it has the highest blood flow. This is what results in a stroke, or stroke. However, embolization can also be anywhere else, causing, for example, acute myocardial infarction, acute necrosis of the intestine or lower limb. Generally, this type of complication is called thromboembolic complication.

The most common thromboembolic complication of atrial fibrillation is stroke
The risk of thromboembolic complications is not the same in every patient. Young and otherwise healthy patients have a very low risk. At the age of 65 and over, the risk rises, and above the age of 75 it is already high. The risk also increases if any of the following conditions are present: high blood pressure (even if the blood pressure normalises with subsequent treatment), diabetes, heart failure or narrowing of the arteries of the heart or lower limbs. And, of course, if the patient has had a thromboembolic event in the past, the risk remains high. Doctors calculate the CHADS-VA score. The higher the score, the higher the risk of stroke in atrial fibrillation. If the score is 2 or more, anticoagulants are given permanently; if the score is 1, their use is on consideration of the bleeding risk. In the case of a score of 0, i.e. in patients younger than 65 years and without any of the risk factors, the risk of thromboembolism is low and the risk of bleeding with anticoagulation treatment outweighs its benefit, so the permanent use of anticoagulants is not recommended in this case. However, irrespective of the risk of thromboembolism, anticoagulants should be given at least three weeks before and one month after procedures such as electrical cardioversion or catheter ablation of atrial fibrillation.

CHA2DS2-VA score. If the score is 0, it is not necessary to take anticoagulants permanently, if it is 1, the recommendation is borderline, if it is 2 or more, it is recommended to take anticoagulants permanently
To calculate the risk of thromboembolic complications, you can use our following calculator:
For long-term anticoagulant treatment, the oral drugs Warfarin or the so-called new oral anticoagulants (NOACs) are used. Warfarin is a classic, time-tested drug, but it has a number of disadvantages. Its treatment must be checked regularly by blood tests and the patient must avoid fluctuations in dietary vitamin K intake. NOACs have less risk of bleeding while maintaining the same protection against stroke. Their treatment does not need to be checked by blood draws and does not require dietary restrictions. Their disadvantage over Wafrarin is that there is an accumulation in reduced renal function. In these cases, their dose must be reduced. There are four NOACs: apixaban, dabigatran, edoxaban and rivaroxaban. All these agents are comparable in terms of efficacy and safety.

The most commonly used anticoagulants. Newly on the market are a number of generic preparations of rivaroxaban and dabigatran.
Another important part of caring for patients with atrial fibrillation is the decision to restore the heart's natural rhythm. The methods that currently exist to restore and maintain natural sinus rhythm have varying efficacy and safety. To date, maintaining a natural rhythm has not been shown to prolong the life of patients compared to those with permanent atrial fibrillation. Thus, when the physician decides whether to adopt a strategy of leaving the arrhythmia and controlling the atrial nodal conduction or fully restoring the natural rhythm, he or she does so on the basis of the patient's difficulties. Older patients with associated diseases may tolerate leaving the arrhythmia well; younger and more active patients often need restoration of natural rhythm to have a good quality of life. If the strategy initially chosen proves inappropriate over time, a second strategy is adopted.

Two basic approaches to treating atrial fibrillation - rhythm control, or trying to restore the natural rhythm, and frequency control, or leaving the atrial fibrillation and trying to slow the ventricular rate
Control of ventricular rate in persistent atrial fibrillation is accomplished with drugs that slow atrial nodal conduction. The most commonly used drugs from the group of beta-blockers are metoprolol and bisoprolol, less frequently from the same group, for example, betaxolol, carvedilol or nebivolol. The calcium channel blocker verapamil or digoxin may also be used. In a small proportion of patients, a permanent pacemaker must be implanted to prevent the heart rate from becoming too slow at times. Conversely, another reason for implanting a pacemaker is too fast a heart rate that cannot be sufficiently slowed by medication. In this case, catheter ablation of the Atrioventricular nodule is then performed at a second time and the patient's atrial impulses are no longer transmitted and the ventricles are permanently stimulated. In this case, the patient is dependent on the pacemaker, therefore, ablation of the Atrioventricular node is performed only when other approaches fail.
Controlling the heart rhythm can be done by a procedure called electrical cardioversion or by administering medication or performing a catheter ablation. Electrical cardioversion is performed under short-term general anaesthesia by means of an electrical discharge through electrodes applied to the chest. The electrical discharge restarts and restores the heart rhythm. The procedure is very safe, but unfortunately does not reduce the long-term risk of arrhythmia recurrence. It can be used when the estimated risk of arrhythmia recurrence is low or if rhythm control drugs or catheter ablation is planned. Sometimes the doctor will recommend cardioversion if the contribution of the arrhythmia to the difficulty is unclear, to see if the difficulty subsides with a normal rhythm.

Electric cardioversion
Rhythm-controlling drugs include propafenone, dronedarone and amiodarone. Propafenone has a rapid onset of action that persists for several hours. It can be used regularly or, in the case of isolated episodes of atrial fibrillation, only once for difficulties. This single-use strategy is called 'pill in the pocket'. The use of propafenone is restricted to patients with normal cardiac function. It must not be used in patients with reduced left ventricular function or chest pain in narrowed coronary arteries because it increases the risk of death. It is therefore more suitable for younger and otherwise healthy patients with only occasional difficulties or when the patient does not wish to undergo catheter ablation. Dronedarone is used less frequently and also cannot be used in patients with reduced left ventricular function. Amiodarone is the most effective of all the drugs. It takes about a month to take effect and the same length of time to wear off after discontinuation. Its administration is safe even in patients with heart failure or chest pain in coronary artery disease. However, the disadvantages are possible side effects with long-term therapy, such as thyroid dysfunction, lung involvement, painful reddening of the skin when exposed to the sun or blurred vision. These side effects must be actively sought after during long-term therapy. After discontinuation of amiodarone, side effects subside, but some may require long-term treatment.

So-called "pill in the pocket" strategy - single use of propafenone 150-300mg tbl for atrial fibrillation
The most effective method for long-term rhythm control is catheter ablation. This is an invasive catheterization procedure performed through a groin approach. After the femoral veins have been tapped, thin tubes are passed through them and then into the right atrium and then through the thin interatrial septum into the left atrium. In the left atrium, ablation, or tissue damage, is performed at the point where the pulmonary veins enter the atrium. The damaged tissue around the veins is then electrically non-conductive and the pulmonary veins are isolated from the atrium, hence this procedure is called 'pulmonary vein isolation' or 'PVI' for short. The entry points of the pulmonary veins are involved in triggering the arrhythmia, and once they are isolated, the arrhythmia can no longer arise so easily. After this procedure, the frequency of atrial fibrillation is reduced, but it can be completely eliminated in the long term in only about 50% of patients. The actual ablation in the left atrium can be done by three methods - point by point using a thin catheter that is heated with radiofrequency energy or by using a freezing balloon that is inflated in the inlets of the pulmonary veins, or by the most currently used method, which is the use of a pulsed field where the tissue is damaged by pulses of high voltage in the inlets of the pulmonary veins. The latter method requires general anaesthesia due to its painful nature, but is faster and safer than the other methods.
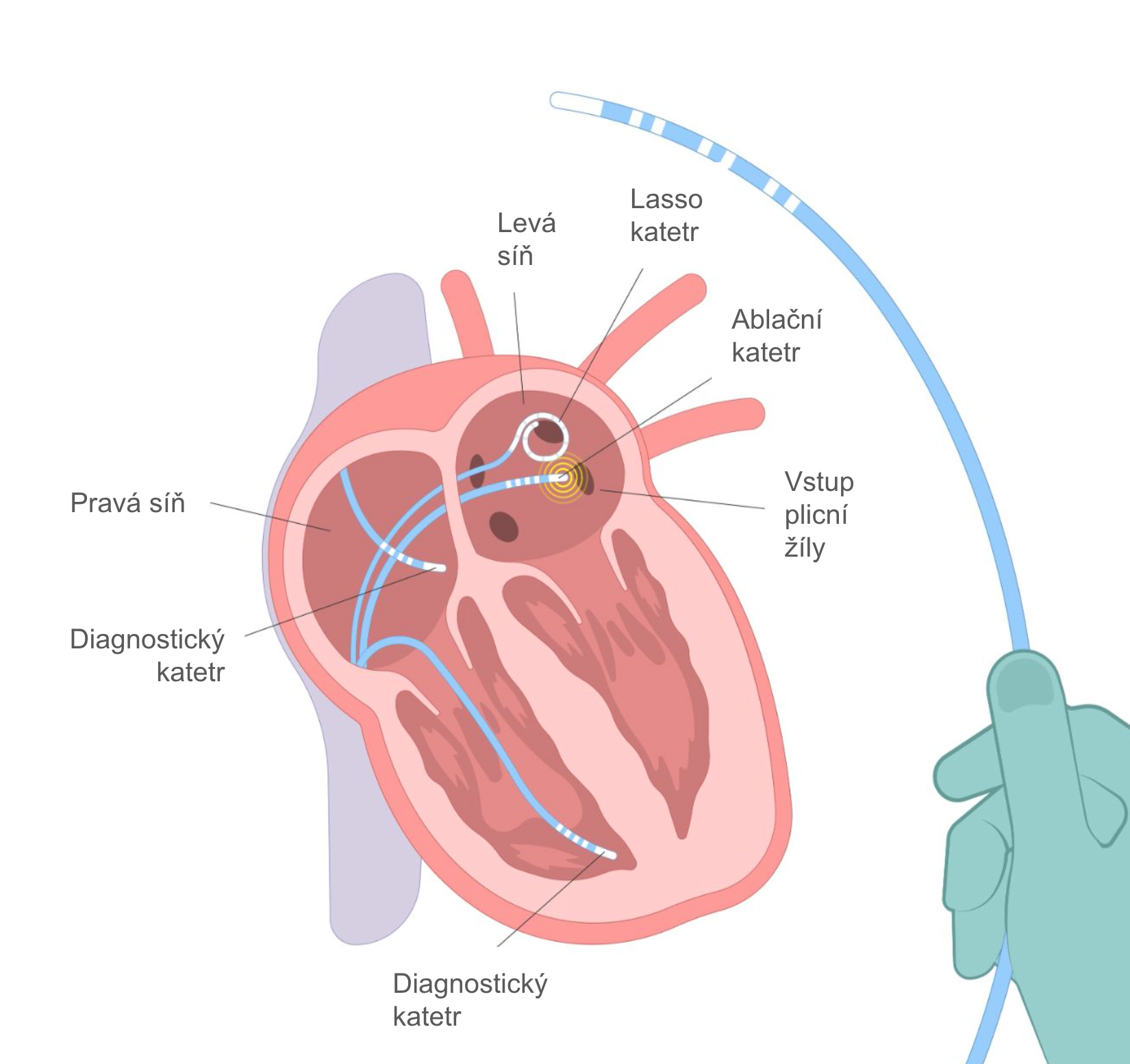
Schematic representation of radiofrequency catheter ablation of atrial fibrillation - isolation of pulmonary veins