CHADSVA
The CHADSVA or CHA2DS2-VA score is based on the previously used CHA2DS2 and CHA2DS2-VASc scoring systems. It indicates the risk of thromboembolic complications in atrial fibrillation. Thromboembolic complications include stroke and embolizations to other arteries of the body, especially to the lower extremities, coronary arteries or the gastrointestinal tract. According to the final score, the doctor decides whether to recommend long-term anticoagulation therapy. The main risk factors are age, a history of stroke, hypertension, diabetes, heart failure and involvement of the arteries of the body, such as the coronary arteries of the heart. The risk is the same for patients with persistent atrial fibrillation as it is for those with a transient form where natural rhythm is restored. The bleeding risk of a given patient should always be considered when deploying.
-
Long-term anticoagulation therapy is not indicated. The risk of bleeding with anticoagulation therapy would outweigh its benefit. However, anticoagulation therapy should be used for at least 3 weeks before and 4 weeks after electrical cardioversion or left atrial catheterisation.
-
It can be individually decided whether to take long-term anticoagulant treatment. In patients at high risk of bleeding, it is better not to use anticoagulation. In patients at low risk, long-term anticoagulation should be considered but is not necessary. However, anticoagulation should be used at least 3 weeks before and 4 weeks after electrical cardioversion or left atrial catheterisation.
-
Permanent anticoagulation therapy is recommended for all patients. In case of recurrent bleeding during anticoagulation treatment, the dose can be reduced or catheterisation of the left atrial appendage can be performed.
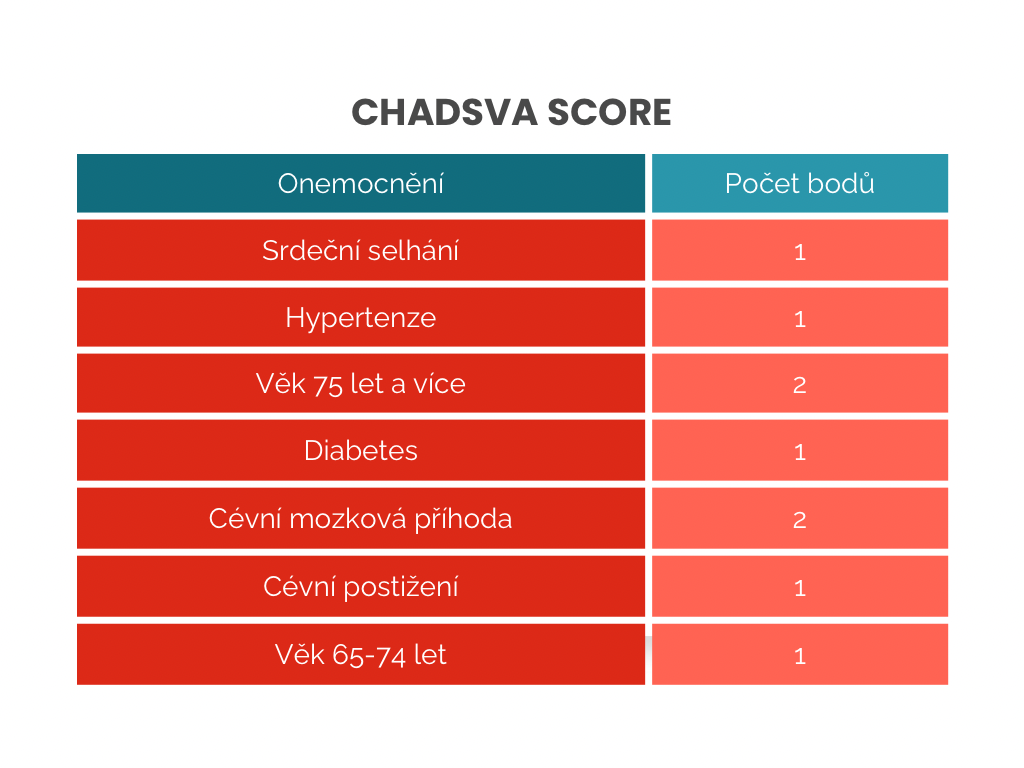
CHADSVA score
Valid regardless of whether atrial fibrillation is permanent or transient. For details, see the Czech Society of Cardiology Recommendations for the Diagnosis and Treatment of Atrial Fibrillation 2024.